HOLAND_CLAIM_FILE_p426
📄 HOLAND_CLAIM_FILE | p.426
📄 HOLAND_CLAIM_FILE | p.426
📝 Extracted Text (OCR)
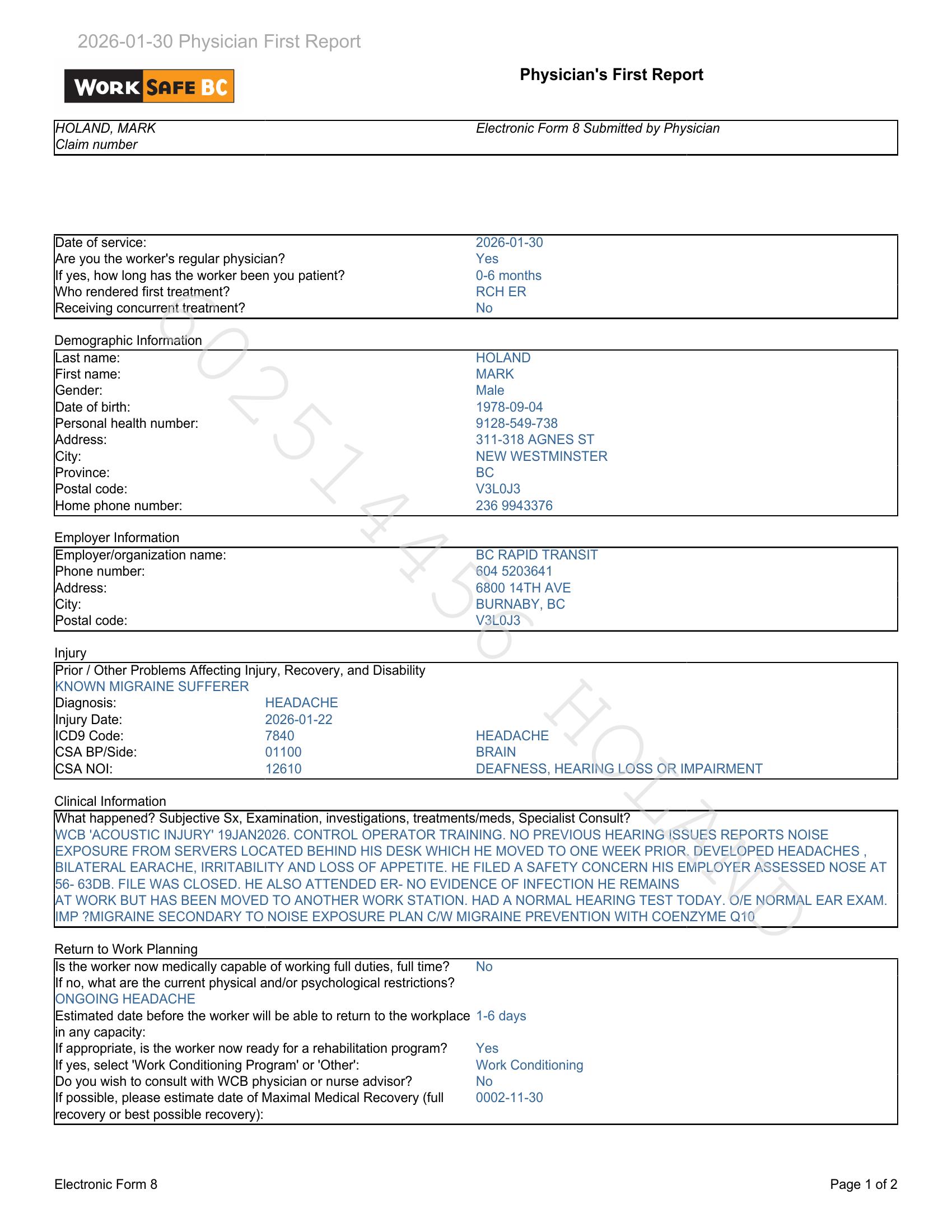
Physician's First Report WORK BC y P IHOLAND, MARK Electronic Form 8 Submitted by Physician Claim number Date of service: 2026-01-30 (Are you the worker's regular physician? Yes lf yes, how long has the worker been you patient? 0-6 months Who rendered first treatment? RCH ER Receiving concurrent treatment? No Demographic Information Last name: HOLAND First name: MARK |Gender: Male Date of birth: 1978-09-04 Personal health number: 9128-549-738 (Address: 311-318 AGNES ST City: NEW WESTMINSTER Province: BC Postal code: V3L0J3 Home phone number: 236 9943376 Employer Information Employer/organization name: BC RAPID TRANSIT Phone number: 604 5203641 (Address: 6800 14TH AVE City: BURNABY, BC Postal code: V3L0J3 Injury Prior / Other Problems Affecting Injury, Recovery, and Disability IKNOWN MIGRAINE SUFFERER Diagnosis: HEADACHE Injury Date: 2026-01-22 ICD9 Code: 7840 HEADACHE ICSA BP/Side: 01100 BRAIN ICSA NOI: 12610 DEAFNESS, HEARING LOSS OR IMPAIRMENT Clinical Information \What happened? Subjective Sx, Examination, investigations, treatments/meds, Specialist Consult? IWCB 'ACOUSTIC INJURY' 19JAN2026. CONTROL OPERATOR TRAINING. NO PREVIOUS HEARING ISSUES REPORTS NOISE EXPOSURE FROM SERVERS LOCATED BEHIND HIS DESK WHICH HE MOVED TO ONE WEEK PRIOR. DEVELOPED HEADACHES , BILATERAL EARACHE, IRRITABILITY AND LOSS OF APPETITE. HE FILED A SAFETY CONCERN HIS EMPLOYER ASSESSED NOSE AT I56- 63DB. FILE WAS CLOSED. HE ALSO ATTENDED ER- NO EVIDENCE OF INFECTION HE REMAINS [AT WORK BUT HAS BEEN MOVED TO ANOTHER WORK STATION. HAD A NORMAL HEARING TEST TODAY. O/E NORMAL EAR EXAM. IMP ?7MIGRAINE SECONDARY TO NOISE EXPOSURE PLAN C/W MIGRAINE PREVENTION WITH COENZYME Q10 Return to Work Planning ls the worker now medically capable of working full duties, full time? No lf no, what are the current physical and/or psychological restrictions? IONGOING HEADACHE Estimated date before the worker will be able to return to the workplace 1-6 days in any capacity: lf appropriate, is the worker now ready for a rehabilitation program? Yes If yes, select 'Work Conditioning Program' or 'Other': Work Conditioning Do you wish to consult with WCB physician or nurse advisor? No If possible, please estimate date of Maximal Medical Recovery (full 0002-11-30 recovery or best possible recovery): Electronic Form & Page 1 of 2