HOLAND_CLAIM_FILE_p413
📄 HOLAND_CLAIM_FILE | p.413
📄 HOLAND_CLAIM_FILE | p.413
📝 Extracted Text (OCR)
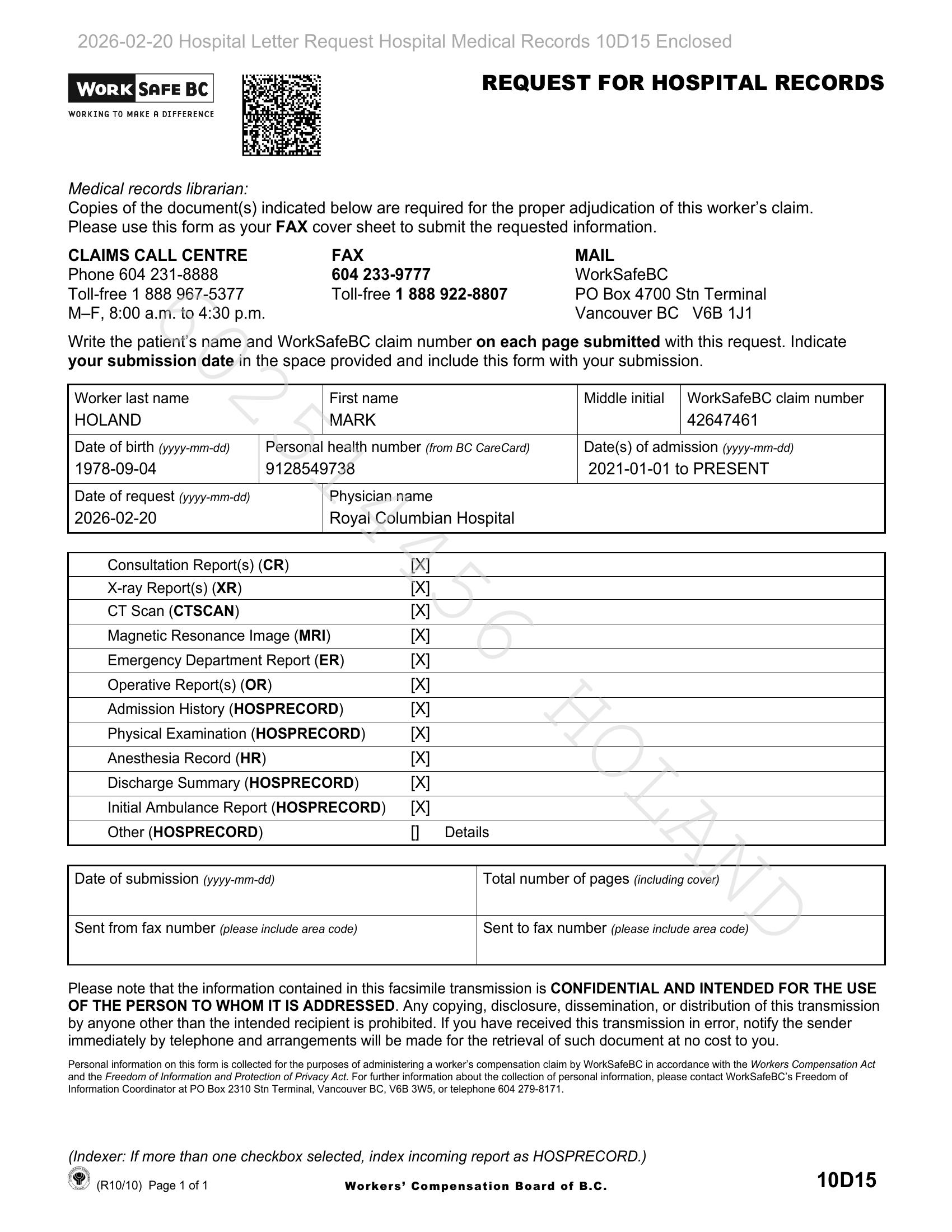
REQUEST FOR HOSPITAL RECORDS | work Eig BC WORKING TO MAKE A DIFFERENCE Medical records librarian: Copies of the document(s) indicated below are required for the proper adjudication of this worker’s claim. Please use this form as your FAX cover sheet to submit the requested information. CLAIMS CALL CENTRE FAX MAIL Phone 604 231-8888 604 233-9777 WorkSafeBC Toll-free 1 888 967-5377 Toll-free 1 888 922-8807 PO Box 4700 Stn Terminal M-F, 8:00 a.m. to 4:30 p.m. Vancouver BC _V6B 1J1 Write the patient's name and WorkSafeBC claim number on each page submitted with this request. Indicate your submission date in the space provided and include this form with your submission. Worker last name First name Middle initial | WorkSafeBC claim number HOLAND MARK 42647461 Date of birth (yyyy-mm-dd) Personal health number (from BC CareCara) Date(s) of admission (yyyy-mm-dd) 1978-09-04 9128549738 2021-01-01 to PRESENT Date of request (yyyy-mm-dd) Physician name 2026-02-20 Royal Columbian Hospital Consultation Report(s) (CR) [IX X-ray Report(s) (XR) [X CT Scan (CTSCAN) [X Magnetic Resonance Image (MRI) [X Emergency Department Report (ER) [X Operative Report(s) (OR) [X Admission History (HOSPRECORD) [X Physical Examination (HOSPRECORD) [X Anesthesia Record (HR) [X Discharge Summary (HOSPRECORD) [X Initial Ambulance Report (HOSPRECORD) = [X Other (HOSPRECORD) 1] Details Date of submission (yyyy-mm-dd) Total number of pages (including cover) Sent from fax number (please include area code) Sent to fax number (please include area code) Please note that the information contained in this facsimile transmission is CONFIDENTIAL AND INTENDED FOR THE USE OF THE PERSON TO WHOM IT IS ADDRESSED. Any copying, disclosure, dissemination, or distribution of this transmission by anyone other than the intended recipient is prohibited. If you have received this transmission in error, notify the sender immediately by telephone and arrangements will be made for the retrieval of such document at no cost to you. Personal information on this form is collected for the purposes of administering a worker's compensation claim by WorkSafeBC in accordance with the Workers Compensation Act and the Freedom of Information and Protection of Privacy Act. For further information about the collection of personal information, please contact WorkSafeBC’s Freedom of Information Coordinator at PO Box 2310 Stn Terminal, Vancouver BC, V6B 3W5, or telephone 604 279-8171. (Indexer: If more than one checkbox selected, index incoming report as HOSPRECORD.) (R10/10) Page 1 of 1 Workers’ Compensation Board of B.C. 10D15