HOLAND_CLAIM_FILE_p401
📄 HOLAND_CLAIM_FILE | p.401
📄 HOLAND_CLAIM_FILE | p.401
📝 Extracted Text (OCR)
Sent 02/23/2026. Weal: 21, Page - 41 Page: 5
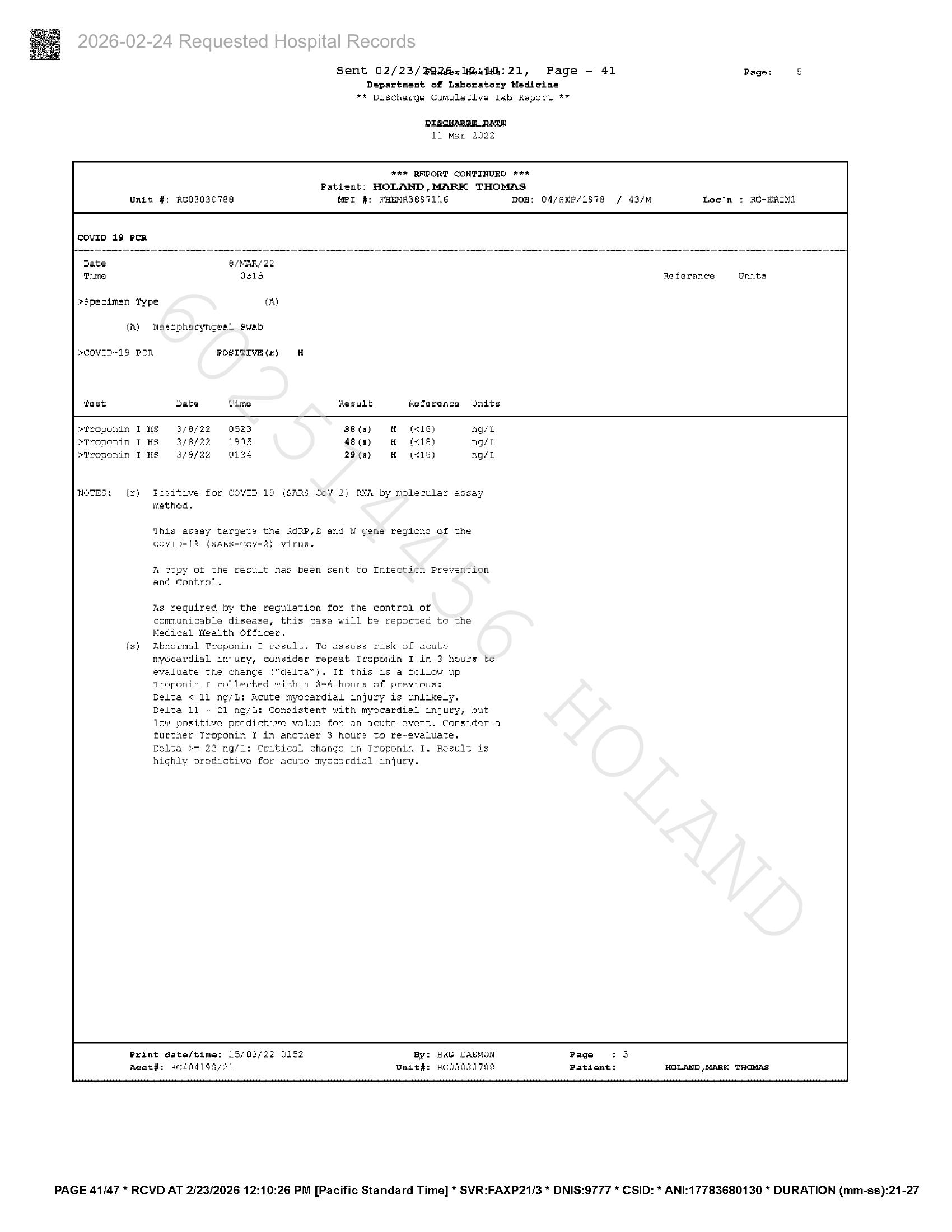
Department of Laboratory Medicine
** Digchacge Cumulative Lab Report **
RIRGHABAR.RALE
Ll Mar 2022
*** REPORT CONTINUED ***
Patient: HOLAND,MARK THOMAS
Unit #: ACO30307398 MPI #: FHEMRS@97116 DOB: O4/saP/1978 / 43/M Loe'n : RU-ERINL
8/MAR/ 22
0815 Re ferance Onits
>Specimen Type (A)
(A) Nasopharyngeal swab
>COVID" 1S POR POSITIVE (%) H
teat Date time Regult Reference Units
etroponin I Ms 3/0/22 0523 3G (a) (<1) ng/t
Troponin I HS 3/8/23 1805 48 (a) (<18) ng/L
eTropornin T HS 379/22 o1a4 25 (a) (18) no/h
NOTES: (£) Positive for CovID-19 (SARS-CoV-2) RNA by molecular assay
method.
This assay target# the RGRP,f and N gene regions of the
COVID-19 (SARS-Cov-2) vicus.
A copy of the result has been sent to Infection Prevention
and Control.
As required by the regulation for the control of
communicable disease, this case will be reported to the
Medical Health officer.
Abnormal Troponin T result. To assess cisk of acute
myocardial injury, consider repeat Treponin I in 3 hours to
evaluate the change ("delta"). If this is a follow up
Troponin I collected within 3-6 hours of previous:
Delta < ll ng/L: Acute myocardial injury is unlikely.
Delta 11 ~ 21 ng/L: Consistent with myocardial injury, but
low positive predictive value for an acute event. consider a
further Troponin I in another 3 hours to re-evaluate.
Delta >= 22 ng/L: Critical change in Troponin I. Result is
highly predictive for acute myocardial injury.
Prdnt date/time: 15/03/22 0152 By: BAG DAEMON Page
Acot#: RCA04198/21 Unit#: RO03020 788 Patient:
PAGE 41/47 * RCVD AT 2/23/2026 12:10:26 PM [Pacific Standard Time] * SVR:FAXP21/3 * DNIS:9777 * CSID: * ANI:17783680130 * DURATION (mm-ss):21-27