HOLAND_CLAIM_FILE_p399
📄 HOLAND_CLAIM_FILE | p.399
📄 HOLAND_CLAIM_FILE | p.399
📝 Extracted Text (OCR)
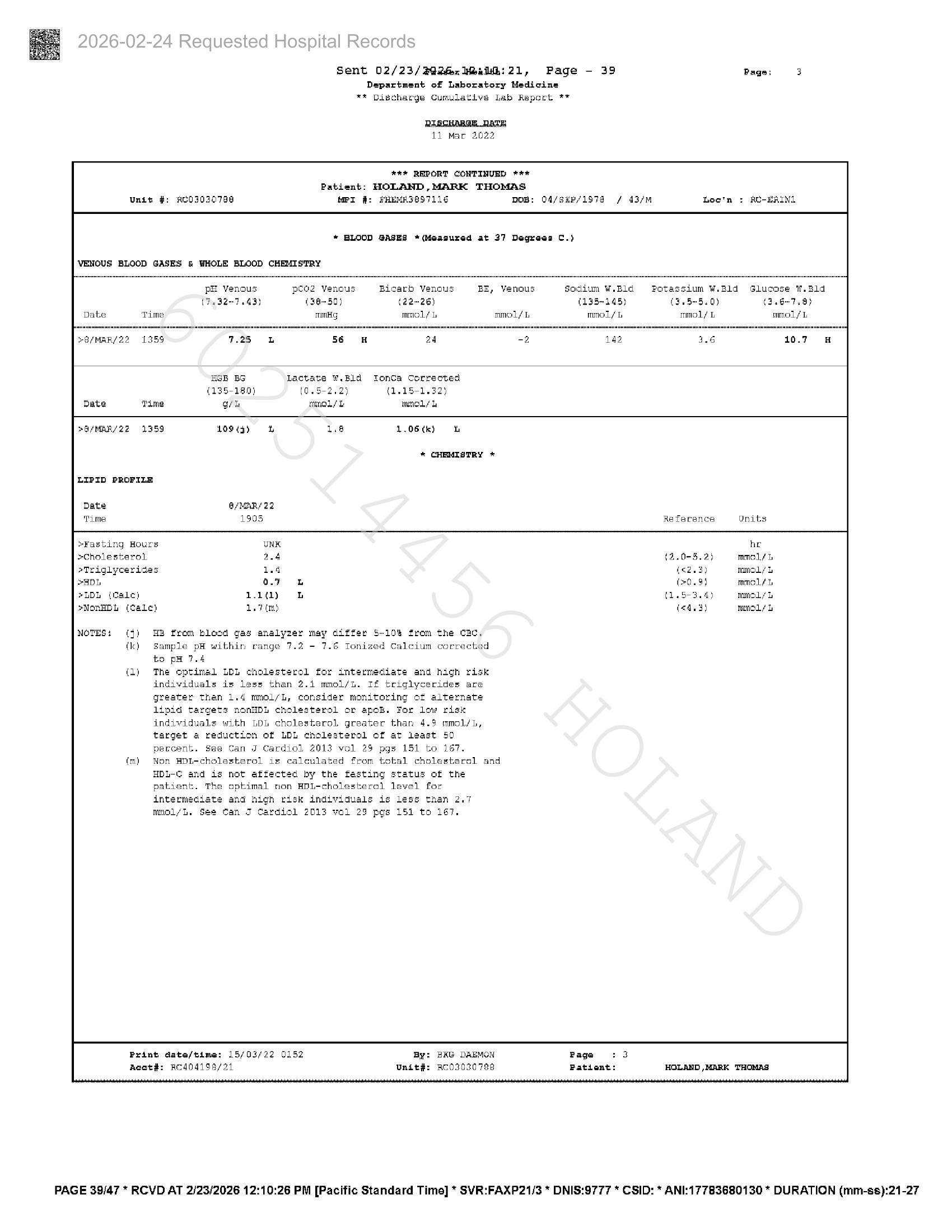
Unit #: ACO30307398 pH! venous Sent 02/23/ @ifex Weal: 21, Department of Laboratory Medicine ** Discharge Cumulative lab Report ** MPI #: FHEMRS@97116 RIRGHABAR.RALE Ll Mar 2022 *** REPORT CONTINUED *** Patient: HOLAND,MARK THOMAS Page - 39 DOB: O4/saP/1978 / 43/M * BLOOD GASES *(Moasured at 37 Degroas C.) VENOUS BLOOD GASES & WHOLE BLOOD CHEMISTRY peoz Venous (7.32-7.43) (38-50) YB/MAR/2Z2 1359 mmHg Bicard Venous BE, Venous (22-26) mmol? lL mmol/L Sodium W.Bld (135-145) mmol/L Loc'n Potassium W.B1d (3.5-5.0) mmol/L Pagan: 3 > RU-BAINI Glucose W.Bld (3.6+7.9) mmol/L Date wie GB BG Lactate Ww. Bld (135-180) (0.5-2.2) gh mmol/l Tonca Corrected (1.15-1.32) mnol/h >O/MAR/Z2 1359 LIPID PROFILE Date Time 10943) i G/MAR/ 22 1903 1.8 1.06 (k) he * CHEMISTRY * Reference »¥asting Hours >CholesterolL Triglycerides SaDL PLDL (Cale) SNonEDL (Cele) UNK a4 1.4 oF 1.11) Le nt) NOTES: (4) HB from blood gas analyzer may differ $-10% from the cad. (k) Sample pH within range 7.2 - 7.6 Tonized Calcium corrected to po 7.4 (1) The optimal LDL cholesterol for intermediate and high risk individuals is less than 2.4 mmol/L. If triglycerides are greater than 1.4 mmol/L, consider monitoring of alternate lipid targets nonHDL cholesterol or apoB. For low risk individuals with LDL cholesterol greater than 4.9 mmol/L, target a reduction of LDL cholesterol of at lsast 50 parcent. See Can J Cardiol 2013 vol 23 pgs 151 to 167. Non HDI-cholesterol is calculated from tokal cholesterol and HDL-¢ and is not affected by the fasting status of the patient. The optimal non HDL-cholesterol level for intermediate and high risk individuals is less than 2.7 mmol/L. See Can J Cardiol 2013 vol 23 pgs 151 to 167. Prant date/time: 15/03/22 0152 Acot#: RCA04198/21 PAGE 39/47 * RCVD AT 2/23/2026 12:10:26 PM [Pacific Standard Time] * SVR:FAXP21/3 * DNIS:9777 * CSID: * ANI:17783680130 * DURATION (mm-ss):21-27 By: Unité: BAG DAEMON BoO3030 788 Page Pationt: (3,.0-5.2) 4<2.3) (>0.9) (165-314) (<4. 3) he mmolé lL mmol/L mmol b mmol/L menos