HOLAND_CLAIM_FILE_p296
📄 HOLAND_CLAIM_FILE | p.296
📄 HOLAND_CLAIM_FILE | p.296
📝 Extracted Text (OCR)
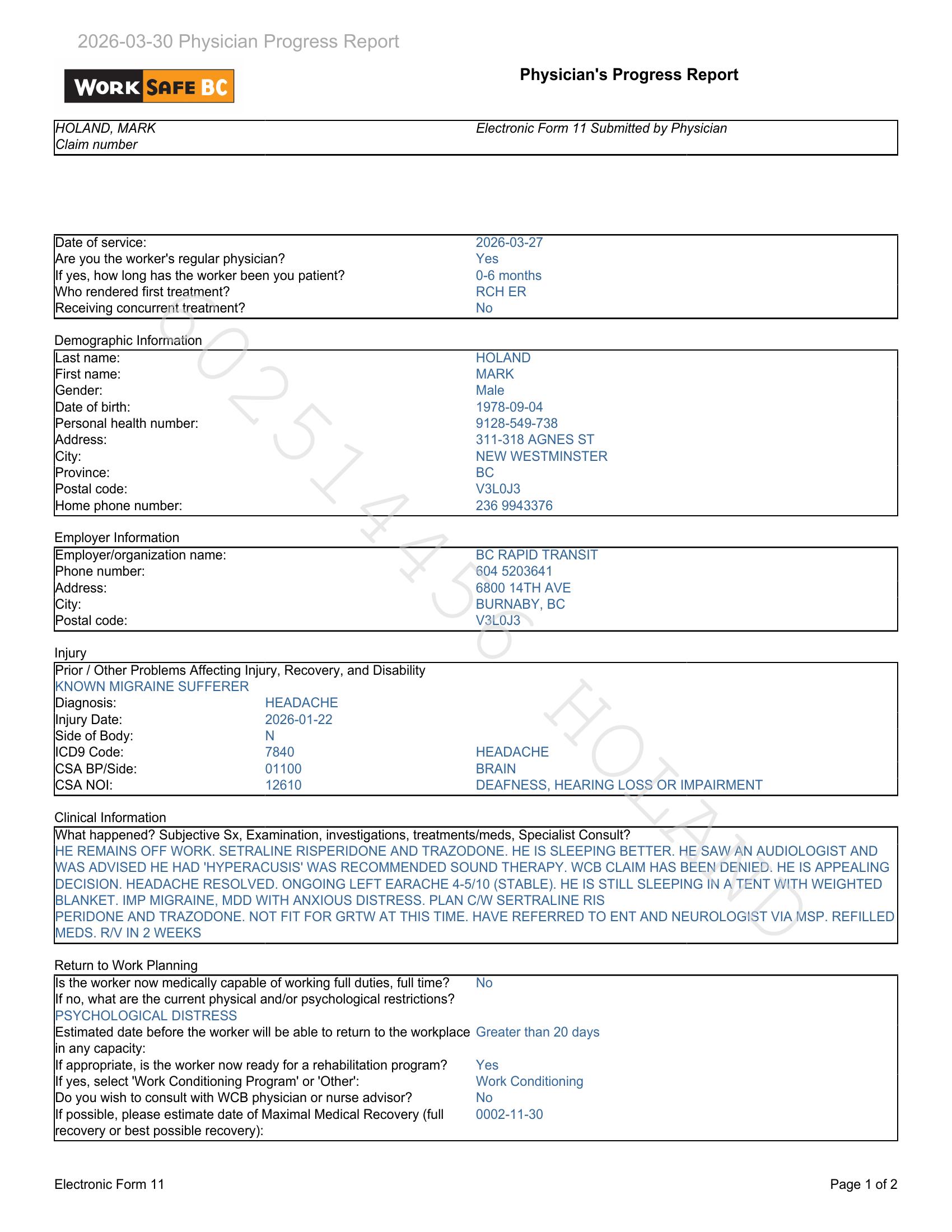
Physician's Progress Report WoRK BC IHOLAND, MARK Electronic Form 11 Submitted by Physician Claim number Date of service: 2026-03-27 (Are you the worker's regular physician? Yes lf yes, how long has the worker been you patient? 0-6 months Who rendered first treatment? RCH ER Receiving concurrent treatment? No Demographic Information Last name: HOLAND First name: MARK |Gender: Male Date of birth: 1978-09-04 Personal health number: 9128-549-738 (Address: 311-318 AGNES ST City: NEW WESTMINSTER Province: BC Postal code: V3L0J3 Home phone number: 236 9943376 Employer Information Employer/organization name: BC RAPID TRANSIT Phone number: 604 5203641 (Address: 6800 14TH AVE City: BURNABY, BC Postal code: V3L0J3 Injury Prior / Other Problems Affecting Injury, Recovery, and Disability IKNOWN MIGRAINE SUFFERER Diagnosis: HEADACHE Injury Date: 2026-01-22 Side of Body: N ICD9 Code: 7840 HEADACHE ICSA BP/Side: 01100 BRAIN ICSA NOI: 12610 DEAFNESS, HEARING LOSS OR IMPAIRMENT Clinical Information \What happened? Subjective Sx, Examination, investigations, treatments/meds, Specialist Consult? IHE REMAINS OFF WORK. SETRALINE RISPERIDONE AND TRAZODONE. HE IS SLEEPING BETTER. HE SAW AN AUDIOLOGIST AND IWAS ADVISED HE HAD 'HYPERACUSIS' WAS RECOMMENDED SOUND THERAPY. WCB CLAIM HAS BEEN DENIED. HE IS APPEALING DECISION. HEADACHE RESOLVED. ONGOING LEFT EARACHE 4-5/10 (STABLE). HE IS STILL SLEEPING IN A TENT WITH WEIGHTED BLANKET. IMP MIGRAINE, MDD WITH ANXIOUS DISTRESS. PLAN C/W SERTRALINE RIS IPERIDONE AND TRAZODONE. NOT FIT FOR GRTW AT THIS TIME. HAVE REFERRED TO ENT AND NEUROLOGIST VIA MSP. REFILLED MEDS. R/V IN 2 WEEKS Return to Work Planning ls the worker now medically capable of working full duties, full time? No lf no, what are the current physical and/or psychological restrictions? IPSYCHOLOGICAL DISTRESS Estimated date before the worker will be able to return to the workplace Greater than 20 days in any capacity: lf appropriate, is the worker now ready for a rehabilitation program? Yes If yes, select 'Work Conditioning Program' or 'Other': Work Conditioning Do you wish to consult with WCB physician or nurse advisor? No If possible, please estimate date of Maximal Medical Recovery (full 0002-11-30 recovery or best possible recovery): Electronic Form 11 Page 1 of 2