HOLAND_CLAIM_FILE_p284
📄 HOLAND_CLAIM_FILE | p.284
📄 HOLAND_CLAIM_FILE | p.284
📝 Extracted Text (OCR)
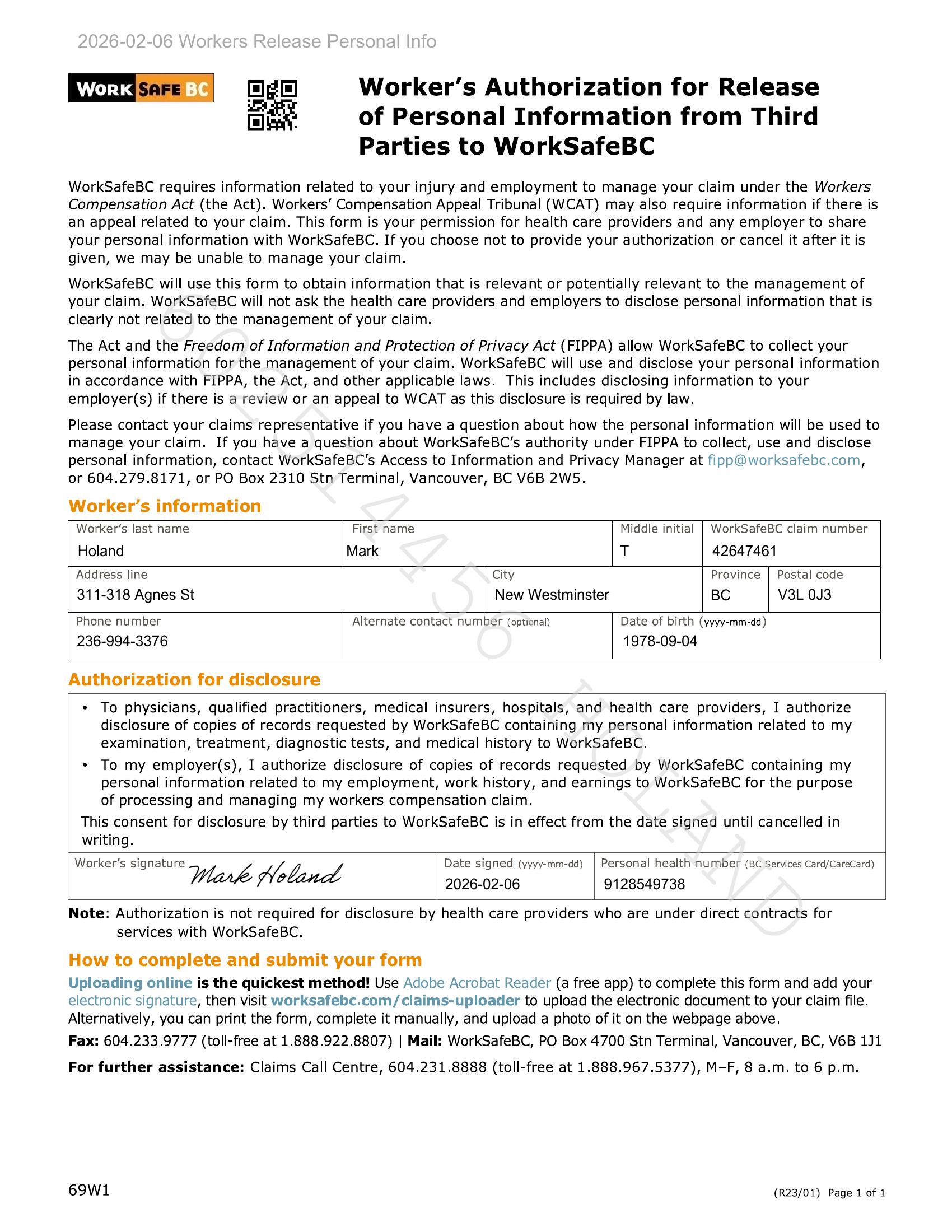
WoRK | work fy BG) a Worker’s Authorization for Release ai of Personal Information from Third Parties to WorkSafeBC WorkSafeBC requires information related to your injury and employment to manage your claim under the Workers Compensation Act (the Act). Workers’ Compensation Appeal Tribunal (WCAT) may also require information if there is an appeal related to your claim. This form is your permission for health care providers and any employer to share your personal information with WorkSafeBC. If you choose not to provide your authorization or cancel it after it is given, we may be unable to manage your claim. WorkSafeBC will use this form to obtain information that is relevant or potentially relevant to the management of your claim. WorkSafeBC will not ask the health care providers and employers to disclose personal information that is clearly not related to the management of your claim. The Act and the Freedom of Information and Protection of Privacy Act (FIPPA) allow WorkSafeBC to collect your personal information for the management of your claim. WorkSafeBC will use and disclose your personal information in accordance with FIPPA, the Act, and other applicable laws. This includes disclosing information to your employer(s) if there is a review or an appeal to WCAT as this disclosure is required by law. Please contact your claims representative if you have a question about how the personal information will be used to manage your claim. If you have a question about WorkSafeBC’s authority under FIPPA to collect, use and disclose personal information, contact WorkSafeBC’s Access to Information and Privacy Manager at fipp@worksafebc.com, or 604.279.8171, or PO Box 2310 Stn Terminal, Vancouver, BC V6B 2W5. Worker's information Worker's last name First name Middle initial | WorkSafeBC claim number Holand Mark T 42647461 Address line City Province | Postal code 311-318 Agnes St New Westminster BC V3L 0J3 Phone number Alternate contact number (optional) Date of birth (yyyy-mm-dd) 236-994-3376 1978-09-04 Authorization for disclosure * To physicians, qualified practitioners, medical insurers, hospitals, and health care providers, I authorize disclosure of copies of records requested by WorkSafeBC containing my personal information related to my examination, treatment, diagnostic tests, and medical history to WorkSafeBC. * To my employer(s), I authorize disclosure of copies of records requested by WorkSafeBC containing my personal information related to my employment, work history, and earnings to WorkSafeBC for the purpose of processing and managing my workers compensation claim. This consent for disclosure by third parties to WorkSafeBC is in effect from the date signed until cancelled in writing. Worker's signature Date signed (yyyy-mm-dd) | Personal health number (BC Services Card/CareCard) Wark Noland 2026-02-06 9128549738 Note: Authorization is not required for disclosure by health care providers who are under direct contracts for services with WorkSafeBC. How to complete and submit your form Uploading online is the quickest method! Use Adobe Acrobat Reader (a free app) to complete this form and add your electronic signature, then visit worksafebc.com/claims-uploader to upload the electronic document to your claim file. Alternatively, you can print the form, complete it manually, and upload a photo of it on the webpage above. Fax: 604.233.9777 (toll-free at 1.888.922.8807) | Mail: WorkSafeBC, PO Box 4700 Stn Terminal, Vancouver, BC, V6B 1J1 For further assistance: Claims Call Centre, 604.231.8888 (toll-free at 1.888.967.5377), M-F, 8 a.m. to 6 p.m. 69W1 (R23/01) Page 1 of 1