HOLAND_CLAIM_FILE_p247
📄 HOLAND_CLAIM_FILE | p.247
📄 HOLAND_CLAIM_FILE | p.247
📝 Extracted Text (OCR)
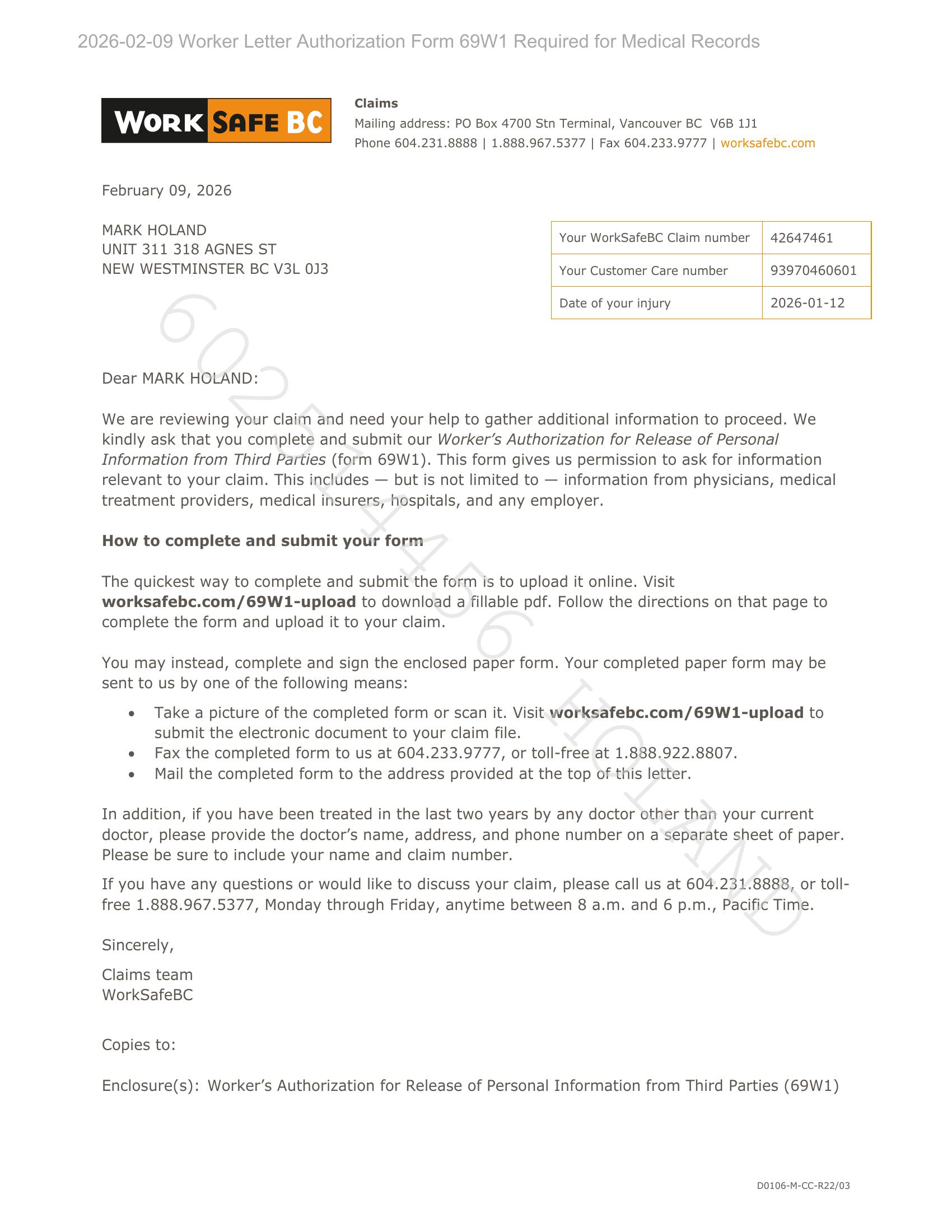
2026-02-09 Worker Letter Authorization Form 69W1 Required for Medical Records Claims WORK BC Mailing address: PO Box 4700 Stn Terminal, Vancouver BC V6B 1J1 Phone 604.231.8888 | 1.888.967.5377 | Fax 604.233.9777 | worksafebc.com February 09, 2026 MARK HOLAND Your WorkSafeBC Claim number | 42647461 UNIT 311 318 AGNES ST NEW WESTMINSTER BC V3L 0J3 Your Customer Care number 93970460601 Date of your injury 2026-01-12 Dear MARK HOLAND: We are reviewing your claim and need your help to gather additional information to proceed. We kindly ask that you complete and submit our Worker’s Authorization for Release of Personal Information from Third Parties (form 69W1). This form gives us permission to ask for information relevant to your claim. This includes — but is not limited to — information from physicians, medical treatment providers, medical insurers, hospitals, and any employer. How to complete and submit your form The quickest way to complete and submit the form is to upload it online. Visit worksafebc.com/69W1-upload to download a fillable pdf. Follow the directions on that page to complete the form and upload it to your claim. You may instead, complete and sign the enclosed paper form. Your completed paper form may be sent to us by one of the following means: e Take a picture of the completed form or scan it. Visit worksafebc.com/69W1-upload to submit the electronic document to your claim file. e Fax the completed form to us at 604.233.9777, or toll-free at 1.888.922.8807. e Mail the completed form to the address provided at the top of this letter. In addition, if you have been treated in the last two years by any doctor other than your current doctor, please provide the doctor’s name, address, and phone number on a separate sheet of paper. Please be sure to include your name and claim number. If you have any questions or would like to discuss your claim, please call us at 604.231.8888, or toll- free 1.888.967.5377, Monday through Friday, anytime between 8 a.m. and 6 p.m., Pacific Time. Sincerely, Claims team WorkSafeBC Copies to: Enclosure(s): Worker’s Authorization for Release of Personal Information from Third Parties (69W1) D0106-M-CC-R22/03