FOI_Release_2026-143_p217
📄 FOI_Release_2026-143 | p.217
📄 FOI_Release_2026-143 | p.217
📝 Extracted Text (OCR)
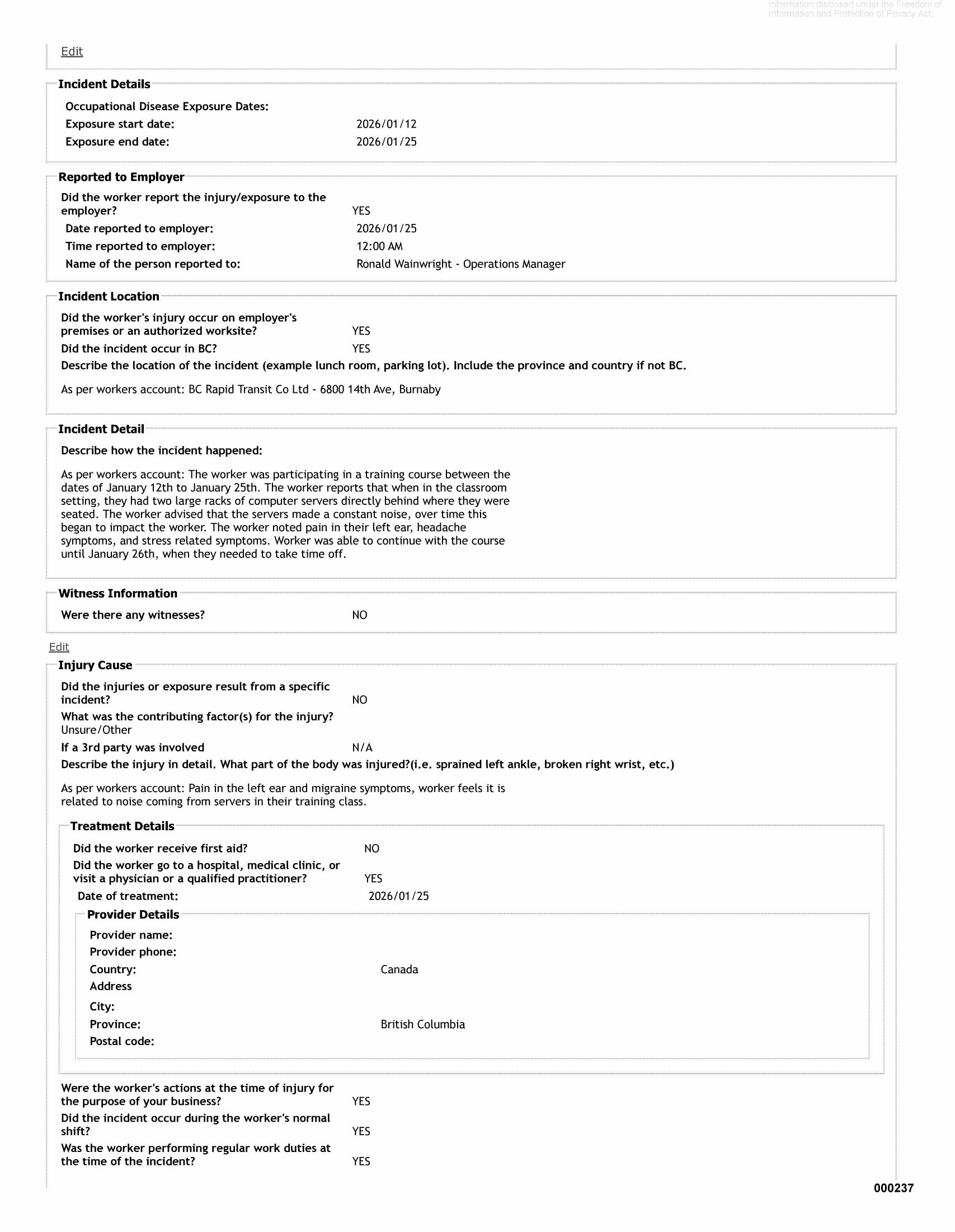
Edit Incident Details Occupational Disease Exposure Dates: Exposure start date: 2026/01/12 Exposure end date: 2026/01/25 Reported to Employer Did the worker report the injury/exposure to the employer? YES Date reported to employer: 2026/01/25 Time reported to employer: 12:00 AM Name of the person reported to: Ronald Wainwright - Operations Manager ~~ Incident Location ~- Did the worker's injury occur on employer's premises or an authorized worksite? YES Did the incident occur in BC? YES Describe the location of the incident (example lunch room, parking lot). Include the province and country if not BC. As per workers account: BC Rapid Transit Co Ltd - 6800 14th Ave, Burnaby Incident Detail Describe how the incident happened: As per workers account: The worker was participating in a training course between the dates of January 12th to January 25th. The worker reports that when in the classroom setting, they had two large racks of computer servers directly behind where they were seated. The worker advised that the servers made a constant noise, over time this began to impact the worker. The worker noted pain in their left ear, headache symptoms, and stress related symptoms. Worker was able to continue with the course until January 26th, when they needed to take time off. Witness Informa‘ Were there any witnesses? NO Edit Injury Cause Did the injuries or exposure result from a specific incident? NO What was the contributing factor(s) for the injury? Unsure/Other If a 3rd party was involved N/A Describe the injury in detail. What part of the body was injured?(i.e. sprained left ankle, broken right wrist, etc.) As per workers account: Pain in the left ear and migraine symptoms, worker feels it is related to noise coming from servers in their training class. Treatment Details Did the worker receive first aid? NO Did the worker go to a hospital, medical clinic, or visit a physician or a qualified practitioner? YES Date of treatment: 2026/01/25 Provider Details Provider name: Provider phone: Country: Canada Address City: Province: British Columbia Postal code: Were the worker's actions at the time of injury for the purpose of your business? YES Did the incident occur during the worker's normal shift? YES Was the worker performing regular work duties at the time of the incident? YES 000237