← Back
📁 MARK'S DOC
Holand00118L_JPG_Completed — p.5
📄 Holand00118L_JPG_Completed | p.5
📄 Holand00118L_JPG_Completed | p.5
📝 Extracted Text (OCR)
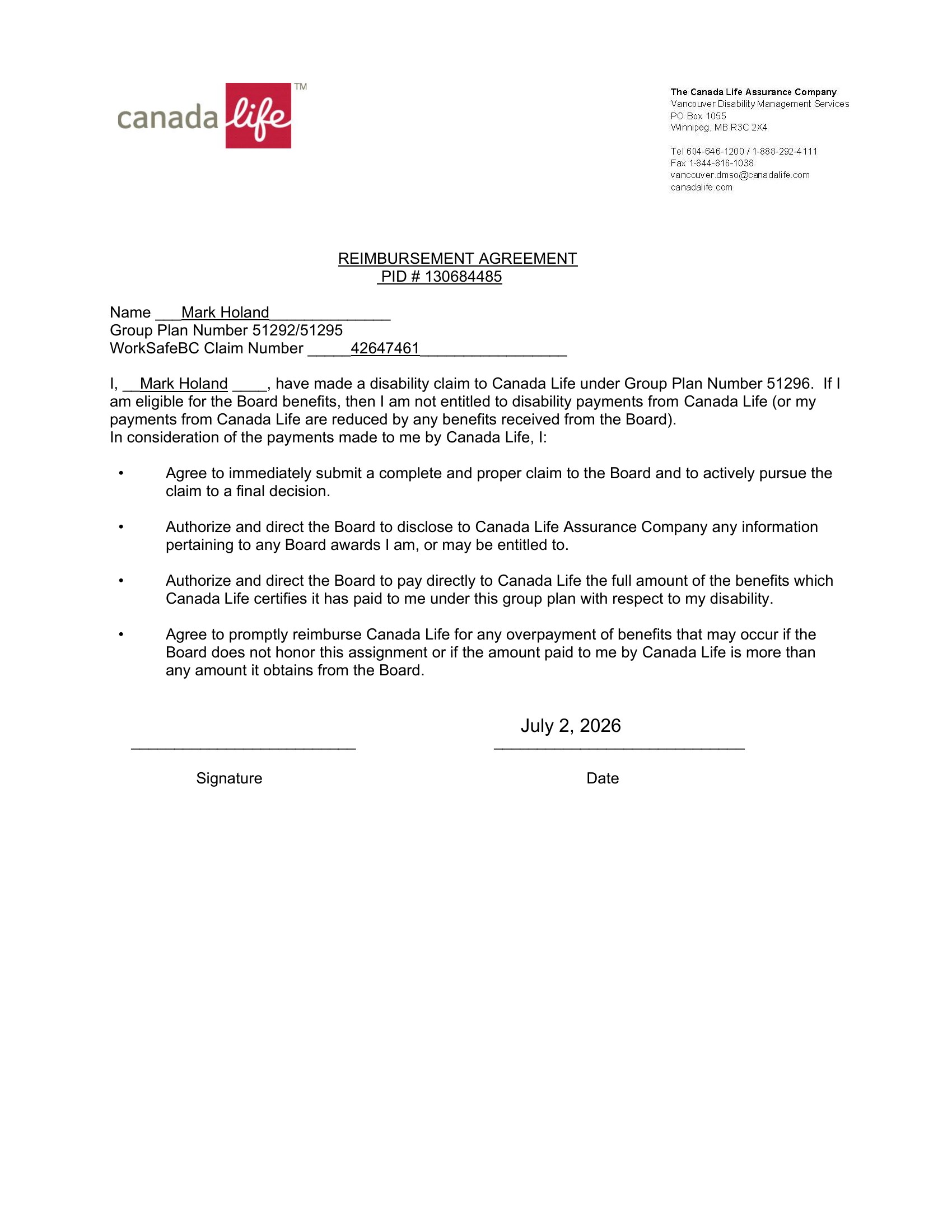
The Canada Life Assurance Company ™ )-f) Vancouver Disability Management Services canada 2 PO Box 1055 aS Winnipeg, MB R3C 2X4 Tel 604-646-1200 / 1-888-292-4111 Fax 1-844-816-1038 vancouver.dmso@canadalife.com canadalife.com REIMBURSEMENT AGREEMENT PID # 130684485 Name Mark Holand Group Plan Number 51292/51295 WorkSafeBC Claim Number 42647461 |, Mark Holand__, have made a disability claim to Canada Life under Group Plan Number 51296. If | am eligible for the Board benefits, then | am not entitled to disability payments from Canada Life (or my payments from Canada Life are reduced by any benefits received from the Board). In consideration of the payments made to me by Canada Life, |: . Agree to immediately submit a complete and proper claim to the Board and to actively pursue the claim to a final decision. . Authorize and direct the Board to disclose to Canada Life Assurance Company any information pertaining to any Board awards | am, or may be entitled to. . Authorize and direct the Board to pay directly to Canada Life the full amount of the benefits which Canada Life certifies it has paid to me under this group plan with respect to my disability. . Agree to promptly reimburse Canada Life for any overpayment of benefits that may occur if the Board does not honor this assignment or if the amount paid to me by Canada Life is more than any amount it obtains from the Board. July 2, 2026 Signature Date