← Back
📁 MARK'S DOC
🔗 Linked Evidence
FOREMED_FAX_MARCH_24-26_4-6 — p.1
📄 FOREMED FAX MARCH 24-26 4-6 | p.1
📄 FOREMED FAX MARCH 24-26 4-6 | p.1
📝 Extracted Text (OCR)
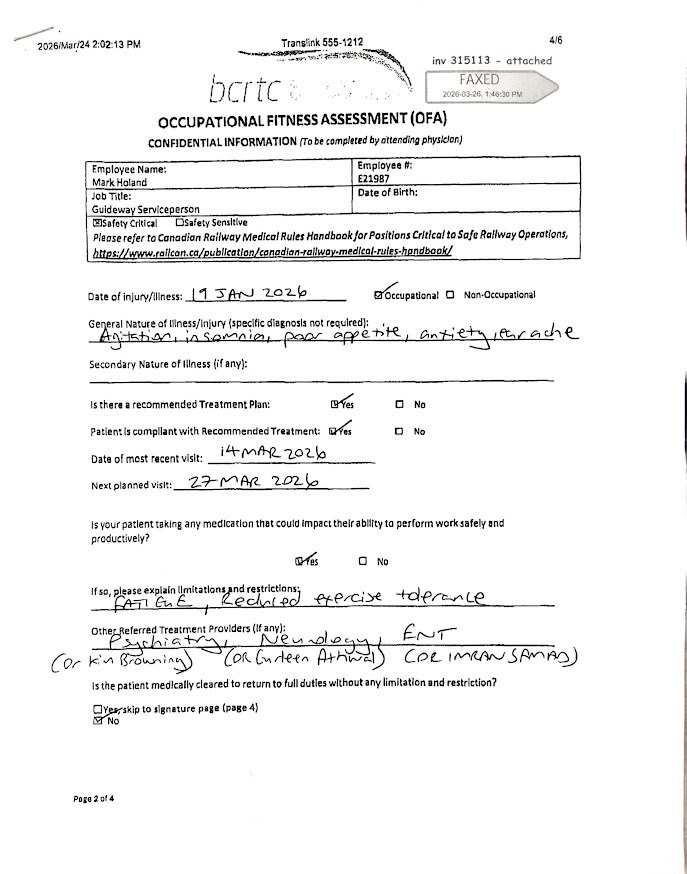
Transcription for: FOREMED_FAX_MARCH_24-26_4-6_p001.txt Source Image: March 24-26 Fax 4-6.jpg Header & Form Data: 1. Top Left Timestamp: 2026/Mar/24 2:02:13 PM 2. Top Middle Header: Translink 555-1212 3. Top Right Page Number: 4/6 4. Fax Stamp: inv 315113 - attached / FAXED 2026-03-26, 1:46:30 PM 5. Form Title: bcrtc OCCUPATIONAL FITNESS ASSESSMENT (OFA) 6. Subtitle: CONFIDENTIAL INFORMATION (To be completed by attending physician) Employee Information: 1. Employee Name: Mark Holand 2. Employee #: E21987 3. Job Title: Guideway Serviceperson 4. Designation: Safety Critical (checked) Medical Assessment (Handwritten & Checked): 1. Date of injury/illness: 19 JAN 2026 2. Category: Occupational (checked) 3. General Nature of illness/injury: Agitation, insomnia, poor appetite, anxiety, headache 4. Is there a recommended Treatment Plan: Yes (checked) 5. Patient is compliant with Recommended Treatment: Yes (checked) 6. Date of most recent visit: 14 MAR 2026 7. Next planned visit: 27 MAR 2026 8. Is your patient taking any medication that could impact their ability to perform work safely and productively? Yes (checked) 9. If so, please explain limitations and restrictions: FATIGUE, Reduced exercise tolerance 10. Other Referred Treatment Providers: Psychiatry (Dr Kim Browning), Neurology (Dr Gurteen Athwal), ENT (DR IMRAN SAMAD) 11. Is the patient medically cleared to return to full duties without any limitation and restriction? No (checked) 12. Footer: Page 2 of 4